
As 12-month prescriptions become available this month, I've been reflecting on what the evidence actually tells us, and whether our instinctive concerns about reduced monitoring might inadvertently harm the patients we're most worried about.
The reticence from our profession is understandable. We worry about lost opportunities for clinical surveillance, about patients drifting for 12 months without a blood pressure check or HbA1c review. These concerns come from a good place. We know that the repeat prescription visits can catch the early hypertensive crisis, the creeping weight gain, the mood change that warrants closer attention.
And yet, while the evidence for harm from access barriers to care is substantial, are our concerns regarding lost opportunistic review valid?
What the data actually shows
Two systematic reviews have examined the evidence on prescription length: King (2018) in the British Journal of General Practice and Miani (2017) for National Institute of Health Care Research. Both searched for studies comparing health outcomes between shorter and longer prescriptions, but found none existed. The concerns we hold about reduced monitoring, while clinically intuitive, have not been tested. What the reviews did find was consistent evidence that longer prescriptions improve medication adherence, with nine out of 13 studies demonstrating benefit and meta-analysis confirming statistical significance.
The adherence question deserves serious attention. US data associates non-adherence with 125,000 deaths annually and 10% of hospitalisations. When patients face barriers to accessing their GP, whether cost, transport, or time off work, they don't fill scripts or they ration medications. The opportunistic care we value becomes unavailable when access barriers mean the patient never presents. In other words, our view is heavily biased toward those patients we see, not those who don’t turn up.
The equity imperative
Prior to this change, New Zealand's three-month prescription limit meant patients faced access barriers in multiples of four each year: four GP fees, four prescription charges, four return trips, four negotiations for time off work. For someone managing multiple chronic conditions, these barriers compound quickly, and they fall hardest on those already facing disadvantage.
Rural patients travel twice the distance for healthcare. Low-income patients weigh medication and consultation costs against food and rent. Māori and Pasifika communities face systemic barriers that accumulate at every point of contact with the health system.
Dr Mataroria Lyndon, whose research is currently examining medicines access, puts it plainly: “Our consultation with underserved communities shows that the cost of seeing a doctor and getting a prescription is a real barrier to care. For whānau managing multiple long-term conditions, these costs add up quickly. Any additional $5 pharmacy charges can further compound the problem. The cumulative effect is rationed medicines, unfilled prescriptions, and avoidable harm - felt most acutely by those with the greatest health needs.”
Prescription length and monitoring are separate decisions
The point often lost in this debate is that prescription length and review frequency are independent variables. A 12-month prescription doesn't mean a 12-month gap in clinical oversight. The RNZCGP already emphasises annual review as the minimum, and this doesn't change.
We retain full discretion to use shorter prescriptions when clinically appropriate. The unstable diabetic, the patient on warfarin, the complex polypharmacy case: these, of course, warrant closer monitoring. But the patient on stable thyroxine and Symbicort for five years, with consistently controlled parameters, is likely better served by reduced access barriers and improved adherence than by quarterly prescription renewals that may or may not involve meaningful clinical review.
It's worth reflecting on how many of our current three-monthly repeats involve genuine, thoughtful, clinical assessment versus a "repeat please" processed between consultations. The safety value of frequent prescriptions exists only when accompanied by actual review.
The money question
There's another factor we don't discuss as openly: practice revenue. Repeat prescription fees represent 7-10% of practice income for many, and the capitation uplift that was meant to offset this change feels inadequate. These are legitimate business concerns in a sector already under financial strain.
But we cannot let business models drive clinical policy that disadvantages vulnerable patients. The path forward requires honest advocacy for sustainable primary care funding, not maintaining access barriers that disproportionately burden those least able to pay.
A both/and approach
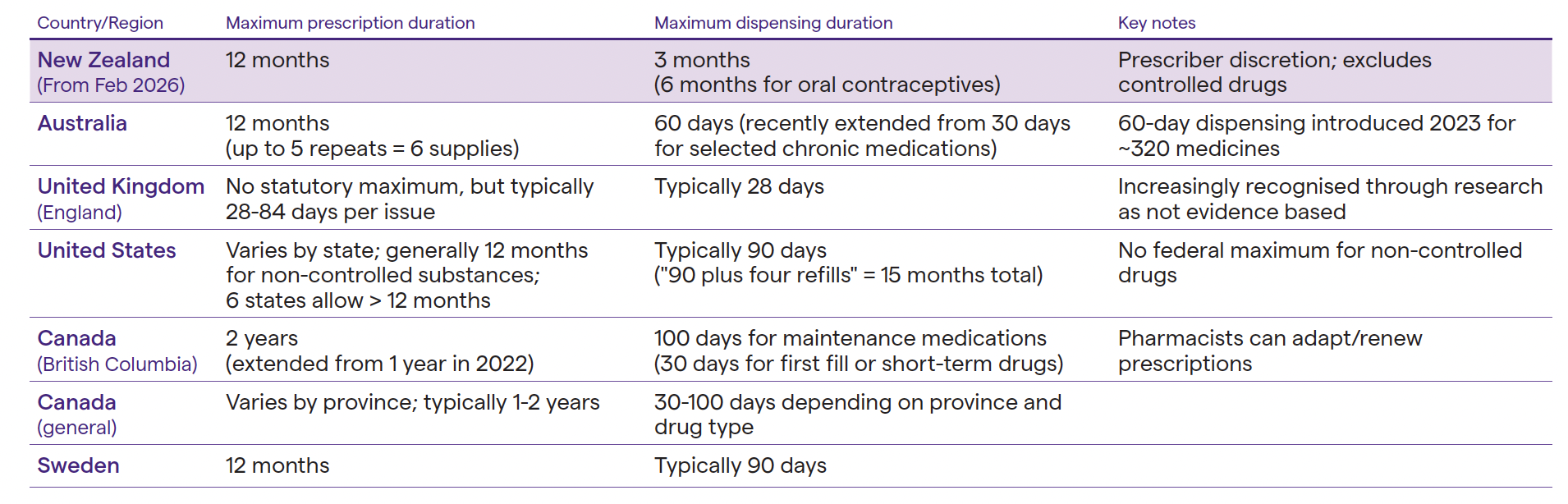
This isn't about abandoning clinical oversight. It's about applying our judgement to determine which patients benefit from which approach. Internationally, Australia, Canada, and most US states have moved to 12-month (or in some cases longer) prescriptions. The UK's 28-day standard is increasingly recognised as an outlier without a strong evidence base.
We have an opportunity to reduce barriers for patients who have struggled to access consistent care: rural communities, working families, Māori and Pasifika whānau managing chronic conditions on tight budgets. The evidence supports this, and our equity obligations demand it. The skill isn't in applying a blanket policy. It's in knowing which patients will benefit from closer monitoring and which are harmed more by access barriers than helped by frequent reviews.
Dr Graham Denyer is the Chief Medical Officer at Tend Health, a board member of Arataki PHO and a member of the New Zealand Medical Assistance Team.