Think about the women in your life. The ones who remember the school notices, organise the family appointments, check in on ageing parents and drop soup to a sick neighbour. They spend so much time caring for others that their own health can quietly slip to the bottom of the list.
For many wāhine, putting themselves first feels like a luxury. But it shouldn't. Every woman deserves to feel listened to, supported and able to access the care she needs.
That's why Tend created Te Wiki Hauora Wāhine | Women's Health Week, returning from 10–16 August. Now in its third year, the nationwide initiative encourages women to make their own health a priority. Throughout the week, we'll be sharing trusted advice from Kiwi health professionals, with each day spotlighting a different topic – from periods and reproductive health to mental health, menopause, cancers, sexual health, fitness and nutrition.
There are free community events, expert webinars, practical health information and prizes to be won, so there's something for everyone.
Plus, as part of Women's Health Week, all Tend clinics are offering free cervical screening for anyone who is due or overdue. Cervical screening is one of the most effective ways to help prevent cervical cancer, yet many women put it off because life gets busy or they feel anxious about the appointment. Our team is here to provide compassionate, respectful care and make the experience as comfortable as possible.
Our kaupapa is simple: to give women permission to put themselves first. Looking after yourself isn't selfish – it's essential. Taking time for your own health means you're better able to keep doing the things, and caring for the people, that matter most.
This August, make yourself a priority. Book that appointment you've been meaning to make, and encourage the women you love to do the same.
Tend Health has launched a suite of web-based services, giving patients browser-based access to primary care - the next step in building New Zealand's most accessible healthcare experience.
Tend has always offered care in two ways: in person at its 15 medical centres across Auckland, Tauranga and Canterbury, and online via the Tend app. Web access is now the third channel in that mix. Patients can request a medical certificate, see a doctor online 24/7, and enrol with Tend - all from a desktop or mobile browser at tend.nz, no download required.
"At Tend, our purpose is to help New Zealanders be the healthiest people in the world, and that means removing every obstacle between a person and their healthcare journey. Our app has been transformative, but it is only one part of a much bigger connected healthcare experience. By bringing together our app, web services, clinics, clinical teams and operational technology into one ecosystem, we can make care easier to access, easier to deliver and more designed around people and their whānau. Web access is our latest contribution to that" says Cecilia Robinson ONZM
The launch comes as New Zealand's health system faces growing pressure from population ageing, workforce shortages and persistent inequities in access to care. The OECD's 2026 Economic Survey of New Zealand identifies digitalisation as a rare, high-potential opportunity - one that can ease those pressures by improving access, reducing administrative burden and lifting productivity. The same report notes that telehealth uptake has improved access overall and web access extends that reach further still.
For some New Zealanders, a smartphone app is not always the most practical way to access healthcare. That might be someone on a laptop, a shared device or a community computer. It might be someone whose vision or dexterity makes a larger device easier to navigate, someone who has no access to a smartphone or has smartphone storage constraints. “Healthcare should fit around people's lives, not the other way around,” says Cecilia
The web services are built entirely in-house by Tend's technology team, expertly led by Chief Operating Officer Josh Robb.
"The app has always been the engine of our digital experience, and the web builds directly on top of it. There are no third-party bolt-ons, no inherited limitations - everything is built to work together. That means we control the security, the design and the roadmap, and we can shape the workflow around our clinical teams and models of care rather than the other way around. When we own the technology, we can respond to what our people on the ground actually need - reducing friction, cutting admin and letting clinicians focus on patients rather than process.
Security is also built in, not bolted-on. Our web services have been externally tested by security specialists and integrate directly with our other systems. Patients can trust that their data is safe. The web and app are fully linked - account information and appointments are consistent across both.
This is the foundation of something much bigger. We want patients to choose how they interact with Tend and for the technology to get out of the way and let them do that," he says.
Tend currently serves 87,000 enrolled patients across its 15 clinics, a patient base that is growing rapidly following the pending acquisition of Green Cross Health's medical division - adding 65 clinics - plus nine clinics through the Better Health Group.
It can be difficult to reconcile the desire for innovation and clinical scale with the deeply human aspects of general practice. For many clinicians, joining a larger organisation often raises the same question: can the values of personal care and connection survive, or even thrive, within a growing network?
The following testimonials from two of our General Practitioners, Dr Paula Taylor and Dr Siobhan Trevallyan, offer an honest look at what that balance actually looks like at Tend. Their experiences highlight how technology and scale can serve, rather than compromise, the essential work of delivering accessible, high-quality patient care.
"I joined Tend in June 2025 as a GP and Group Clinical Director for the Bay of Plenty, and I know that joining a large organisation can feel like a step into the unknown. So I want to share honestly what it is really like to be part of this team.
Yes, Tend is a large organisation. But it is an organisation that genuinely lives by its purpose. Tend was founded with a vision to transform healthcare for current and future generations, and that shows up every day in two ways: a real commitment to equitable, accessible care for patients, and an equally real commitment to looking after the people who deliver it. Tend understands that a sustainable business is built by caring for the teams within it, and you feel that.
Tend is an innovator, using technology to improve the experience of both patients and clinicians. It is also a collaborator. Your opinion is wanted and your voice is heard, from frontline teams through to the executive. Everyone, from the CEO to contractors, is expected to live up to our values, our Tendencies, and they do. I remember my first visit to the head office, when I met our Co-CEO, Cecilia Robinson. She was polishing the office windows and vacuuming the floor, simply part of the team. That humility has stayed with me.
People here are valued for what they bring, and contributions are openly celebrated across the whole company. There is a genuine sense of fairness. I have worked in small GP owned practices and in large corporations, and Tend is the first place I have found where scale and values truly sit together. Not everything always goes to plan, and Tend is not afraid to acknowledge that and change direction when needed. That honesty matters.
I can also speak personally. Since my cancer diagnosis, Tend has looked after me with flexibility, generosity and real care. It is one thing to read an organisation's values on a website; it is another to feel them when life gets hard. There is collaboration across Tend clinics nationwide, and despite our size it feels like a family rather than a corporate organisation. I am proud of being part of this team."
Dr Paula Taylor General Practitioner & Clinical Director - Bay of Plenty
"I have been working with Tend as both an in-clinic and online General Practitioner since 2024, and it has been one of the most rewarding professional experiences of my career.
One of the greatest strengths of working with Tend is the flexibility it offers. The ability to combine in-person and virtual consultations, alongside flexible working hours, allows me to provide high-quality care while maintaining a sustainable work-life balance. This flexibility benefits not only clinicians but also patients, improving access to healthcare in ways that are increasingly important in modern general practice.
What stands out most about Tend is its unwavering focus on patient care, access, and clinical outcomes. Decisions are consistently guided by what will deliver the best experience and health outcomes for patients.
The organisation has invested heavily in digital tools that genuinely enhance clinical practice, streamlining workflows, supporting continuity of care, and enabling clinicians to spend more time focused on patients rather than administrative tasks.
The breadth and depth of the clinical network is another significant advantage. Working alongside a large and diverse group of clinicians creates a remarkable hive of knowledge, experience, and support. Whether discussing complex cases, sharing insights, or learning from colleagues across the country, there is a strong sense of collaboration and collective expertise.
During my time with Tend, I have been impressed by the organisation’s commitment to innovation and continuous improvement. Tend has evolved significantly, but change is never implemented for its own sake. New initiatives are thoughtful, reflective, and deeply embedded within a robust clinical quality framework. This creates confidence that innovation is being pursued responsibly, with patient safety and quality care remaining at the forefront.
Tend is an organisation that values its clinicians, embraces innovation, and remains steadfastly committed to delivering accessible, high-quality healthcare. I am proud to be part of its journey."
Dr Siobhan Trevallyan Lead for Tend Kingsland and Tend Symonds St - Auckland
As published in The New Zealand Herald, Saturday 27 June 2026
It is not often that meaningful change in New Zealand’s health system happens quietly.
Health is usually loud. It is political, personal and often understandably emotional. When things go wrong, they are felt quickly by patients, families, clinicians and communities. The pressure points are visible: long waits, stretched hospitals, difficulty getting a GP appointment, workforce shortages and the frustration people feel when the system does not work as it should.
But when things improve, progress can be harder to see. It can happen in policy settings, improved data collection and reporting, funding formulas, targets, operating models and infrastructure. Right now, there are some positive changes happening in health that deserve to be acknowledged. They are not perfect. They will not fix decades of underinvestment overnight. But they are progressing. In a system as complex as health, progress matters.
One of the most important changes is the overhaul of the way primary care is funded.
For nearly 20 years, New Zealand has used a capitation formula that has been widely accepted as too blunt. Capitation is the base funding general practices receive for enrolled patients, but the old model reduced a highly diverse population to just twelve possible funding amounts based on gender and six broad age bands. It did not properly reflect the reality that different patients, whānau and communities have very different levels of health need.
That matters because funding design drives behaviour. If funding does not reflect need, then the system risks underfunding the very communities that require more care, more outreach and more support. This is why the reweighting of capitation is important.
The new formula is not perfect. Ethnicity has not been included as a variable, which remains a significant issue given the persistent inequities experienced by Māori and Pacific peoples. There will also be winners and losers in any redistributive model.
But after two decades of talking about the need for change, the system has moved.
Credit should go to health officials and Health Minister Simeon Brown for progressing this important work. Overhauling a 20-year-old funding model is difficult and politically brave, particularly when any reweighting inevitably creates trade-offs. Audrey Young recently described Brown as “focused”, and this is a clear example of that focus being put to work on something that matters.
Nationally, Health New Zealand is investing an additional $128.4 million into primary care as part of this change. That matters. The reweighting is not just an academic exercise in funding design; it is backed by real investment into the part of the system where earlier care can make the biggest difference.
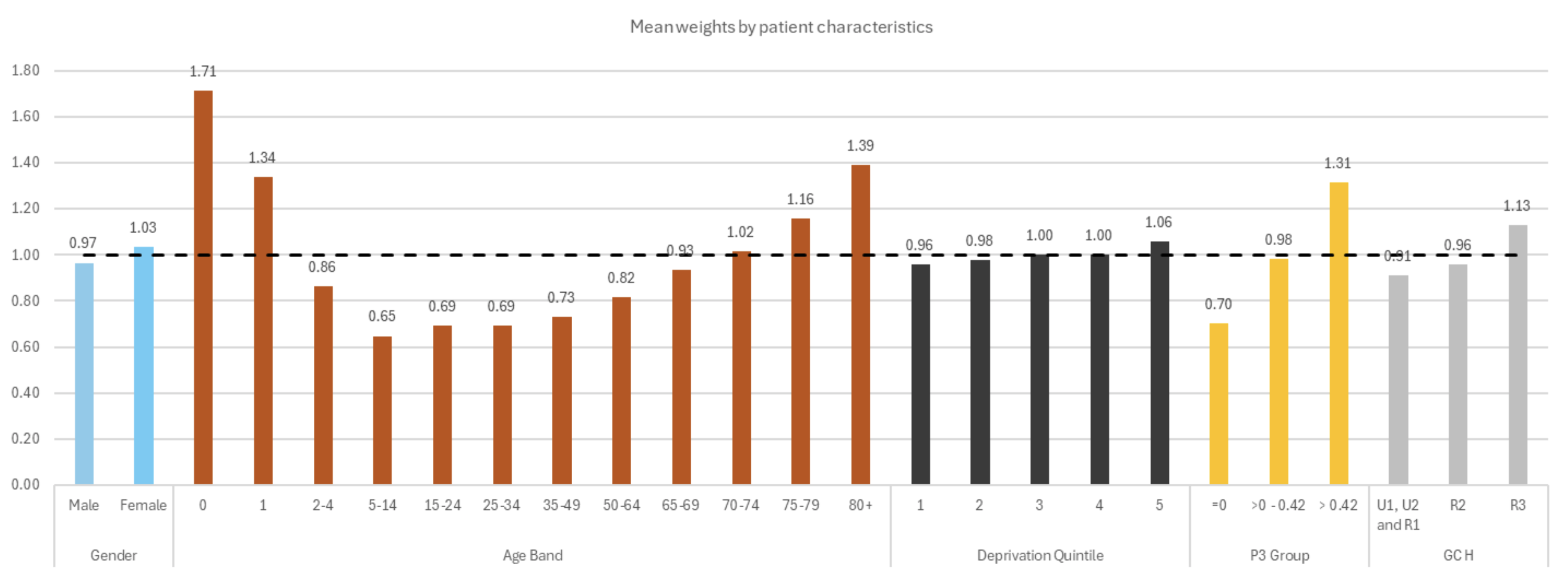
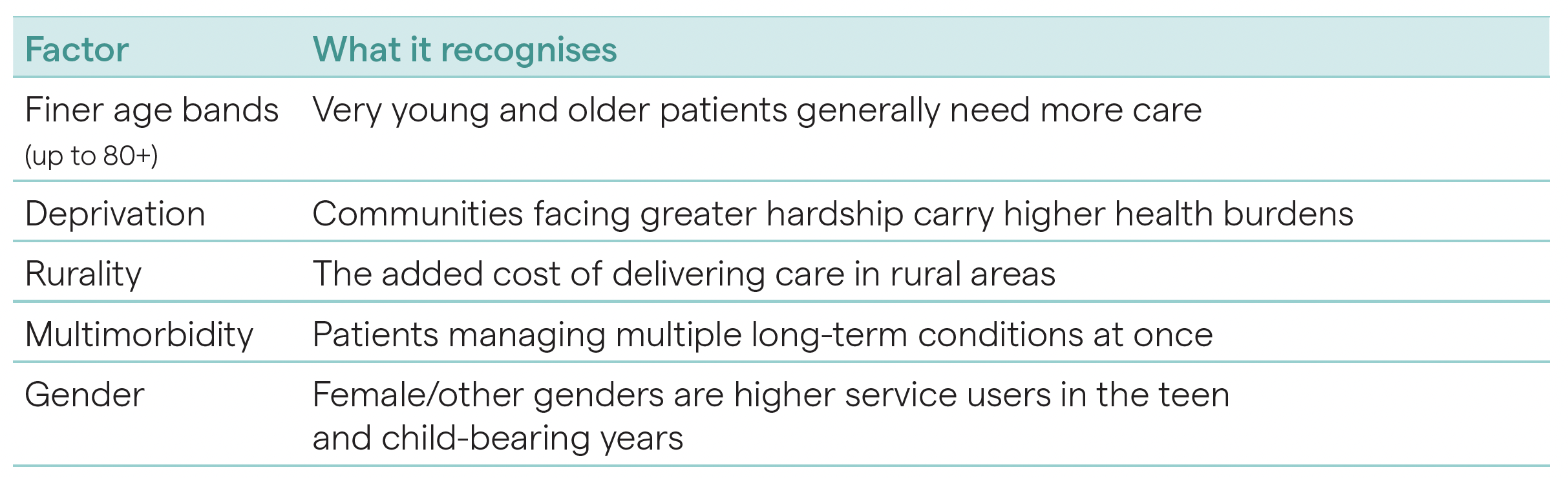
The new approach takes account of more detailed age bands, deprivation, rurality and multimorbidity, creating 1,080 different funding combinations. While that may sound complex, it means funding can be more precisely targeted to need. That is a meaningful shift towards funding care based on the complexity of patients’ lives, not simply the number of people enrolled.
It recognises that an 80-year-old with multiple long-term conditions may require far more care, follow-up and support than a generally healthy 65-year-old. It recognises that rural communities face different access challenges. And it recognises that deprivation has a direct impact on health outcomes, and should therefore be reflected in how care is funded.
That should be welcomed. It is also notable how little noise there has been around this change.
Often, health reform is accompanied by loud opposition, competing interests and sector tension. This change could easily have generated significant pushback because any reweighting of funding is, by definition, redistributive. Yet the relative lack of noise may reflect a quiet acceptance that the old system was no longer fit for purpose.
Primary care is the front door of the health system. It is where prevention happens. It is where early diagnosis happens. It is where chronic conditions are managed, medications are reviewed, children are immunised, mental health issues are first raised and many health problems are dealt with before they become hospital admissions.
When primary care works well, the whole system benefits. Patients get care earlier. Families have fewer crises. Hospitals are less pressured. Health outcomes improve over time. Properly funding primary care is not just good for general practice; it is one of the best investments we can make in the long-term sustainability of New Zealand’s health system.
The economics are clear. Keeping someone in a hospital bed overnight can cost around $7,000. Earlier intervention in primary care can often be delivered at a fraction of that cost, sometimes close to a tenth. That might mean treating an infection before it escalates, managing a chronic condition earlier or supporting someone before they end up in emergency care. It is better for patients, better for whānau and better for the taxpayer.
This is why primary care should not be seen as the cheap end of the health system. It is the smart end of the health system. It is where relatively small investments can prevent much bigger human and financial costs later. This also matters in the context of the Government’s health targets.
Targets are not the whole answer. They can never capture the full humanity of healthcare or the complexity of patient need. But they do provide clarity. They tell the system what matters and where effort needs to be focused.
The current health targets focus on faster cancer treatment, improved childhood immunisation, shorter stays in emergency departments, shorter waits for first specialist assessments and shorter waits for elective treatment. These are areas that matter deeply to New Zealanders. The latest results show year-on-year improvement across all five targets. The job is not done: too many New Zealanders are still waiting too long, and access remains uneven. But progress should not be dismissed simply because pressure remains. Both can be true.
There is also a new primary care access target due to take effect from July 2026. That is important. If we are serious about improving health outcomes, access to primary care needs to be measured, managed and improved with the same discipline as hospital performance. A strong health system starts much earlier. It starts with reminders, recalls, screening, immunisation and proactive care. It starts with services that are easy for people to use, including people who have historically found the system hard to navigate.
That is why primary care reform matters so much. We should be honest about the scale of the challenge. But we should also be honest when progress is being made. The shift in capitation funding, the focus on measurable health targets, increased investment in general practice, the development of online and after-hours options and work on shared health records all point to a health system slowly starting to modernise.
The real test will be execution.
Funding must reach the frontline. Targets must improve outcomes, not just reporting. Digital care must expand access without fragmenting continuity. Equity must be built into the system, not added later. And primary care must be treated as core infrastructure for New Zealand’s future health, not simply a pressure valve for hospitals.
In health, it is easy to focus only on what is broken. We must keep calling out gaps, delays and inequities, but we should not miss the moments where the system is beginning to shift.
Overhauling a 20-year-old funding system is progress. Clearer targets are progress. More investment in primary care is progress. Recognising patient need more accurately is progress. Modernising access to care is progress.
None of it is enough on its own, but it is a start. The challenge now is to keep going: to build on the momentum, keep improving the model, ensure funding supports communities with the greatest need and keep primary care at the centre of the health system we need for the future.
New Zealanders deserve a health system that is easier to access, more equitable, more connected and more focused on keeping people well.
We are not there yet. But some of the foundations are beginning to move in the right direction, and that should give us reason for optimism.
Tend Health today announced it has entered into an agreement to acquire the medical division of Green Cross Health Limited, which operates general practice and urgent care clinics under The Doctors brand.
When completed, the transaction will bring together Green Cross Health’s established medical network of 65 medical centres, trusted local clinical teams and Tend’s innovative primary healthcare technology platform.
James Robinson, Co-CEO and Co-Founder of Tend Health, said: “This is an important moment for Tend and, when completed, for the future of primary care in Aotearoa me Te Waipounamu (New Zealand). The Doctors is a well-established community healthcare provider, with strong relationships across the communities they serve. Our focus is on enhancing care and health outcomes, while supporting continuity for patients, clinical teams and local communities.
“With the backing of iwi and other leading New Zealand investors, Tend has the opportunity to maintain local ownership of this important primary care infrastructure, while continuing to build a long-term healthcare business focused on supporting access, improving patient health outcomes and sustainable primary care.”
Ngāi Tahu Holdings, an existing shareholder in Tend, is supporting the proposed transaction and will increase its shareholding in Tend, with Ngāti Whātua Ōrākei also increasing its stake as a key iwi partner and shareholder, alongside new shareholder Nāti Growth and existing shareholder Ahuahu Group.
Together, this reflects strong iwi investor support for Tend’s long-term growth, with iwi investors becoming one of Tend’s largest shareholder groups alongside a broader base of leading New Zealand investors and existing shareholders.
It represents a strong New Zealand investment group backing Tend’s next stage of growth, supporting local ownership and our long-term purpose to help New Zealanders be the healthiest people in the world.
Tend’s technology-enabled model has supported more convenient, connected patient experiences across its existing network, including improved access to care for high-needs patients, while keeping trusted clinical relationships and patient care at the centre.
Todd Moyle, Chief Executive of Ngāi Tahu Holdings, said, “Ngāi Tahu Holdings is excited to support a New Zealand owned business that is building a technology enabled platform to improve access, patient experience and health outcomes.
“Over the past few years, Tend has continued to invest in technology that supports primary care, with a focus on improving access, patient experience and continuity of care”.
Lisa Davis, Chief Executive of Ngāti Whātua Ōrākei, said: “Ngāti Whātua Ōrākei is proud to support Tend’s next phase of growth alongside Ngāi Tahu Holdings, Nāti Growth and other Aotearoa me Te Waipounamu investors. We’re already seeing positive impacts through our partnership with Tend and are excited about what could be achieved together in the future.
“We see primary care as critical social infrastructure, and this proposed acquisition reflects our commitment to long-term investments that are responsive to the needs of whānau, communities and patients across the motu.”
Cecilia Robinson, Co-CEO and Co-Founder of Tend Health, said: “This is about building for the long term. Primary care is one of the most important parts of our health system, with a vital role in prevention, early identification of health concerns and helping our people stay well.
“Within the next 20 years, it is projected that one in three tamariki in Aotearoa me Te Waipounamu will identify as Māori. That is why we believe strong iwi and Māori partnerships matter deeply for the future of health in New Zealand.
“It will also build on our partnership with Ngāti Whātua Ōrākei, increase Ngāi Tahu Holdings’ shareholding in Tend and bring Nāti Growth alongside other leading local investors supporting the next stage of Tend’s growth.
“We are also grateful for the continued support of existing shareholders, who have backed Tend’s long-term vision for primary care in Aotearoa me Te Waipounamu.
“For us, this is about purpose and people. Tend was founded to help New Zealanders be the healthiest people in the world, and our people remain at the heart of everything we do. We have enormous respect for the legacy of The Doctors, and for the clinical teams who have built trusted relationships with patients and communities over many years.
“Our focus is on supporting that legacy while continuing to invest in the future of primary care in Aotearoa me Te Waipounamu. This is an opportunity to build a 100-year Kiwi-owned healthcare business for future generations.”
Transaction details
The transaction is subject to Green Cross Health shareholder approval. The transaction is expected to be completed by 31 July, subject to that approval being received. Green Cross Health shareholders will receive a notice of meeting for that approval in due course.
In the early days of my work as a Health Improvement Practitioner (HIP), I was nervous about implementing what was then a radically new approach to mental health intervention. The model emphasised brief, focused session - often just one or two contacts, typically 30 minutes long - a stark contrast to the traditional therapeutic models I had practised and taught for more than 25 years. Like many of my peers, I questioned whether such brief interactions could deliver meaningful change. Those concerns quickly faded in practice. I was able to provide immediate support to more people, often on the same day, delivering interventions that were both focused and effective.
A national programme takes shape
The outcomes from the New Zealand HIP pilot were compelling, and these early results led to the development of the Integrated Primary Mental Health and Addiction (IPMHA) HIP programme. This programme now includes more than 700 HIPs working across New Zealand primary care clinics, representing a major shift in the delivery of mental health care. The model demonstrated that brief, focused interventions could produce powerful results, enabling clinicians to reach a much larger number of people while still facilitating meaningful and lasting change.
Taking the model digital
This brief behavioural change approach has now moved into the digital space. Tend Health launched its funded digital mental health service in September 2025, as part of The Mental Health and Addiction Community Sector Innovation Fund. Through the Tend app, anyone in New Zealand can book a fully funded 30-minute structured consultation with a Health Improvement Practitioner. There is no referral, no enrolment, and no payment required. The service operates weekdays from 8am to 8pm.
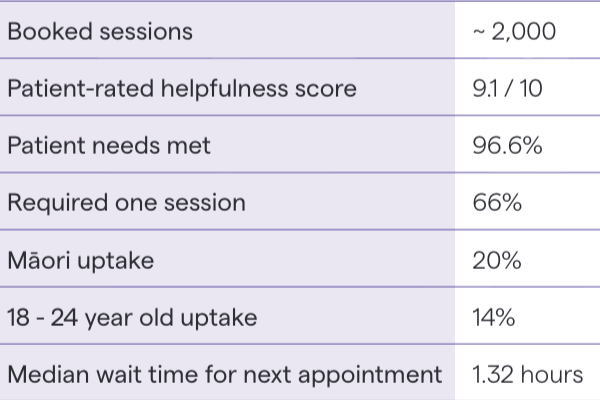
The usual in-person HIP approach has been enhanced with Tend's online video technology, dedicated customer support teams, and real-time data and metrics to support clinical governance. Since launch, the service has recorded close to 2,000 booked appointments, demonstrating growing demand for a low-barrier national mental health pathway.
" The accessibility and responsiveness of the HIP approach is proving to be highly valuable - not only for patients but also for my primary care colleagues, who benefit from having rapid, practical mental health support integrated into their teams. "
While the number of appointments is lower than our original forecast, that forecast assumed a higher proportion of people would need multiple visits. What we are actually seeing is very positive for an early intervention model: around two-thirds of patients are getting the support, guidance and next steps they need in a single appointment, and our patient experience and intervention metrics are very strong. That tells us the service is reaching the right people, at the right time, in a way that is genuinely helping.
These early results are encouraging, particularly when measured against our core objectives of helpfulness and accessibility. To date, we have achieved an average patient-rated helpfulness score of 9.1/10, with 96.6% of patients reporting that their specific needs were met. From an accessibility perspective, the next available appointment has always been within the same day (median time to next available appointment is 1.32 hours).
Expanding reach and access
In recent months, as the service has moved into the scale-up phase, we have increased our focus on reaching underserved communities - students and tertiary providers, rainbow communities and rural sector workers. Almost one in five patients identifies as Māori, and 14% are aged 18-24, suggesting the service is reaching priority groups who often face greater barriers to timely mental health care. We are also beginning to collect wellbeing outcome data through the WHO-5 measure. Early results show the service is predominantly reaching people with mild to moderate wellbeing concerns, which is the intended cohort for this model of care.
The service is drawing patients from across New Zealand, including both enrolled and non-enrolled patients, reinforcing the value of a national digital access pathway. The team currently includes five Health Improvement Practitioners and myself. Every patient receives a succinct summary and behavioural change plan minutes after the consultation, and a full set of clinical notes is provided to their GP via the usual clinical channels. Where additional support is needed, our team provides recommendations and liaises with the person's own GP and in-clinic HIP, or refers on to other services, including stepping up to specialist mental health care when required.
What the results have taught me
Reflecting on those early doubts, I now see this as an incredibly rewarding way of working. I'm impressed by how New Zealand has adopted high-fidelity clinical approaches, like Focused Acceptance and Commitment Therapy (FACT), to deliver such effective, outcomes-focused interventions. The integration of new technology has been a genuine shift, significantly reducing the administrative burden on clinicians and improving patient reach. Using a telehealth platform explicitly designed to simplify primary care workflows allows us to focus less on paperwork and more on the people we serve. By weaving these digital tools directly into our daily processes, we are finally increasing access to care across the wider population.
My initial concerns about a lack of depth have been answered by the tangible results I see every day. I am so proud of the impact we are making, driven by a team that is genuinely kind and focused on improving the wellbeing of our communities. We have finally found a way to balance clinical sophistication with a model that actually meets the scale of the need.
Ōrākei Health becomes Tend Ōrākei in partnership with Ngāti Whātu. Ōrākei in May - our fourteenth clinic integration, and our first in partnership with iwi. But what does integration into the Tend network actually mean?
The conversation usually starts with technology. Indici. Clinical inboxes. AI scribing. The Tend app. Phone systems. Email. But after thirteen integrations we know that technology changes, while stressful, are not where the real challenges lie.
What we're doing is relatively unique in New Zealand general practice. This isn't a corporate roll-up where practices keep their own systems and standards while capitation flows to a parent entity. We fully integrate: one practice management system, one clinical governance framework, one technology platform, one data lake, one set of standards. That distinction matters because it means integration isn't a transaction. It's a culture change. And it requires genuine investment - not just in technology, but in our teams - to drive improvement for clinicians, patients and frontline staff.
What we find when we look closely
That culture change starts with visibility. When you bring practices onto a single platform with consistent clinical standards and transparent reporting, you see everything - including things that weren't visible before.
We have integrated practices that were high-performing, well-run and clinically strong. We have also, in the course of integration, discovered issues that had been hidden or unrecognised - in some cases serious. This is not a criticism of the people involved. It reflects a sector where some practices have operated in relative isolation, often without the systems or support to identify problems early. RNZCGP Foundation Standard is exactly that - a foundation.
I believe this transparency is one of the most important things we offer. You cannot improve what you cannot see. A quality and consistency lens applied across a network reveals patterns - both good and concerning - that it is difficult for any single practice, however well-intentioned, to identify in isolation.
The human cost of change
None of this diminishes the reality that integration is demanding. When a GP has spent fifteen years navigating the same system, built their own shortcuts, established their own rhythms with their team, asking them to change all of that is not a technology challenge. It is a psychological one. Tasks that once required no conscious thought suddenly demand active effort. And on thesame day the system changes, the clinic gets a new name, new patient channels and new processes. The simultaneity is significant.
We don't minimise this; we resource it. Our integration programme starts ten weeks before go-live: hardware audits, process mapping, in-clinic visits, progressive training and four hours of dedicated hands-on preparation the day before migration. For the first three weeks after, experienced Tend staff are physically on-site - GPs supporting GPs, nurses supporting nurses, admin supporting admin. These are people who have recently been through an integration themselves. Their presence is as much solidarity as supervisory. Dedicated app concierges work from the waiting room for two months, ensuring patients get unhurried support so admin staff are not expected to absorb that load on top of everything else.
Twelve months, not twelve weeks
The structured programme runs for weeks. The real adjustment takes twelve months or more. The operational improvements are measurable early. Our Central Clinical Team takes over repeat prescribing from day one, delivering a 56% reduction in administrative burden within the first month. Patient satisfaction always rises. A GP at one of our practices described her first post-integration leave as the first proper holiday she'd had in her career. The cultural shift takes longer. Learning to work within a network rather than as an autonomous unit. Accepting that transparent data will surface things that may be uncomfortable. Building trust that our purpose is genuine and the support structures are sustained. These are changes measured in months and quarters, not days.
A sample of outcomes post integration
Feedback from a recent integration
"To the superstars who have been our support crew, navigators, moral support and amazing new colleagues, a heartfelt thank you from the new Tend team in the South Island! Without you we would not have got through the past few weeks. Your honesty about this journey, letting us know there will be bumps and that days would be challenging, were wise words. A whole new world has been opened up to us. Thank you and we look forward to our Tend journey ahead!" - Nurse Lead Kirsty Sidebottom
Why this matters
We are not building a chain. We are building a network with shared standards, shared systems, and a shared commitment to quality and equity, with strong local leadership and decision making. That requires more than technology adoption. It requires a willingness to be open about what is working and what is not.
If you are a practice owner or clinical leader considering this conversation, I can tell you that the first months are demanding. But they are supported, structured and closely held. And the teams who have come through it consistently describe what follows as better - for them, for their patients, and for their working lives
Thirteen integrations in, we know what works. More importantly, we know it takes longer than any programme can deliver. The programme gets you through the transition. The culture is what makes it stick.
When a measles outbreak tested our ability to identify and reach unvaccinated patients within 48 hours, the answer wasn't more staff. It was better data.
I'm not a clinician. My background is in technology, product and engineering leadership, most of it outside healthcare entirely. When I co-founded Tend Health six years ago, I expected the clinical complexity of primary care. What I didn't expect was the state of the data systems underpinning it.
After two decades building data platforms in financial services and SaaS, walking into the primary care sector was confronting. Incomplete patient records fragmented across incompatible systems. Population health queries that should take minutes requiring months of manual work. Risk stratification that in any other regulated industry would be automated, being done on spreadsheets, or not done at all. This isn't a criticism of the people working in the sector. It reflects decades of under investment in the infrastructure that sits beneath clinical care. I’ve often said that our digital health infrastructure is in a considerably worse state than Middlemore's often cited plumbing.
Six months into Arataki PHO's operation (established to contract directly with Health New Zealand on behalf of Tend's network) we're beginning to see what is possible when that infrastructure gap is addressed. Two recent examples illustrate the point.
Immunisation in Bay of Plenty
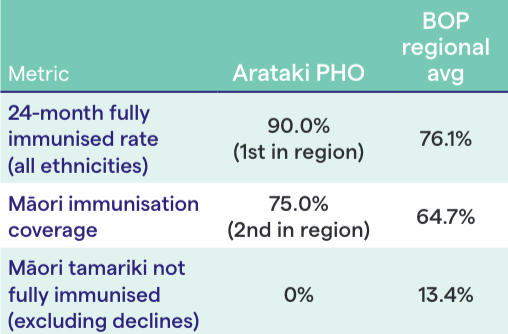
Bay of Plenty (BOP) has recorded some of the lowest immunisation rates in Aotearoa for years, making it a persistent focus for Health New Zealand's System Level Measures (SLM) programme. At the quarterly SLM review in February 2026, the data from Arataki's practices was striking.
Our BOP practices achieved the highest 24-month fully immunised rate in the region across all ethnicities: 90% against a regional average of 76%. Māori immunisation coverages at at 75%, second in the region. And Arataki was the only PHO in Bay of Plenty with no Māori tamariki classified as not fully immunised (excluding firm declines).
These results didn't come from a single campaign. They reflect consistent, data-informed prioritised outreach: knowing which tamariki are due, which whānau need follow-up, and which communities face the greatest access barriers. That requires a data platform that surfaces answers in real time, not quarterly. The clinical teams did the work. The data infrastructure made sure they were reaching the right patients at the right time.
Measles response: directive to doorstep in 48 hours
That infrastructure was tested more acutely in October 2025 when measles re-emerged in Nelson with 11 confirmed cases, seven linked to a Bluebridge ferry crossing. Health New Zealand directed all PHOs to urgently boost vaccination rates.
Within 24 hours a multidisciplinary data and clinical team had built tools to identify unvaccinated patients stratified by risk: prioritising children under five, Māori and Pacific youth and people in high-deprivation areas. Within 48 hours, frontline nurses had prioritised lists in hand and were planning outreach. This wasn't a generic broadcast. It was targeted, evidence-led and fast.
The outreach was multi-channel: clinician-led video content in Te Reo Māori, English, and Mandarin; a patient messaging campaign achieving a 61% open rate; community partnerships; and walk-in immunisation clinics in high-needs areas including Eastgate Mall in Linwood, Christchurch.
The results above were measurable. Weekly MMR vaccinations rose from 32 per week to 189, a 5x increase. Conversions among previously vaccine-hesitant patients increased by 2.5x. And external vaccination records updated in practice management systems increased by 17x, reflecting a significant improvement in the data quality underpinning all future outreach.
"These results aren’t stories about one PHO performing well - they’re evidence of what becomes possible when primary care treats data as a crucial clinical tool, not just a reporting obligation. You can only close a gap when your systems are good enough to reveal it." - Josh Robb
The systemic gap this reveals
That last number matters more than it might appear. The measles response surfaced a significant challenge: adult vaccination records, particularly for overseas arrivals, are frequently incomplete or inaccessible. This isn't an Arataki problem - it's a sector-wide one. But you can only identify a data gap when your systems are good enough to reveal it.
This is the broader point. The sector's capacity challenges are real and well documented: workforce shortages, rising chronic disease burden, half a million New Zealanders not enrolled with a GP. Our ability to respond to these challenges depends fundamentally on data and digital infrastructure that most of the sector still lacks, particularly at the clinical frontline.
The investment required isn't glamorous. It's multidisciplinary teams with data engineering, system integration, analytics capability and the clinical knowledge and workflows that connect population-level insight to individual patient action. It's the kind of investment that health as historically undervalued compared to every other regulated industry I've worked in. But without it, we're making decisions within complete information, reacting to crises rather than anticipating them and measuring outcomes long after the opportunity to change them has passed.
Bay of Plenty's immunisation results and the measles response aren't stories about one PHO performing well. They're evidence of what becomes possible when primary care treats data as a crucial clinical tool rather than a reporting obligation.
On Wednesday evening, after a very short illness, we lost Dr Lee Mathias ONZM, a pioneering leader whose impact on healthcare in Aotearoa New Zealand has been profound and enduring.
Over more than four decades, Lee helped shape the way healthcare is delivered in this country. She was a nurse first and foremost, beginning her career at Middlemore Hospital and rising to become Principal Nurse. That grounding stayed with her throughout her life. She never lost sight of the critical role nurses and frontline teams play, consistently championing and empowering them as the foundation of a stronger, more equitable health system.
Lee’s impact on healthcare in New Zealand is both wide-reaching and lasting. As the founder of Birthcare (her PhD) and Labtests, she transformed maternal care and diagnostic services — creating supportive, woman-centred environments and building infrastructure that set new standards for care delivery in Aotearoa.
Her broader influence on New Zealand’s healthcare system through her governance roles shaped policy and practice in ways that continue to benefit patients today. As Chair of Counties Manukau District Health Board and Deputy Chair of Auckland District Health Board, she was a strong advocate for health equity, championing initiatives that addressed the needs of under-resourced communities.
Across her wider governance roles, including the Health Promotion Agency, Medicines New Zealand and numerous public and community organisations, she consistently advanced more equitable access to care and better health outcomes for all New Zealanders.
Lee was also a founding director and investor in Tend Health, where she played a central role in building a modern, patient-centred model of care that continues to serve communities across the motu. From day one, Lee backed our vision and invested in our purpose of helping New Zealanders be the healthiest people in the world. Her influence extended beyond healthcare into business and leadership, where she was a tireless advocate for women and an inspiring mentor to many.
Lee’s legacy is one of courage, razor wit, innovation and deep compassion. She leaves behind a healthcare system that is stronger, more accessible and more equitable because of her life’s work.
Our thoughts are with her sons Jack and Matt, their families and grandchildren, her husband Rob, all her whānau, and all those who had the privilege of working alongside her.


%20(2).jpg)
.jpg)

%20(3).jpg)

.jpg)
.png)

.jpg)