.jpg)
When a measles outbreak tested our ability to identify and reach unvaccinated patients within 48 hours, the answer wasn't more staff. It was better data.
I'm not a clinician. My background is in technology, product and engineering leadership, most of it outside healthcare entirely. When I co-founded Tend Health six years ago, I expected the clinical complexity of primary care. What I didn't expect was the state of the data systems underpinning it.
After two decades building data platforms in financial services and SaaS, walking into the primary care sector was confronting. Incomplete patient records fragmented across incompatible systems. Population health queries that should take minutes requiring months of manual work. Risk stratification that in any other regulated industry would be automated, being done on spreadsheets, or not done at all. This isn't a criticism of the people working in the sector. It reflects decades of under investment in the infrastructure that sits beneath clinical care. I’ve often said that our digital health infrastructure is in a considerably worse state than Middlemore's often cited plumbing.
Six months into Arataki PHO's operation (established to contract directly with Health New Zealand on behalf of Tend's network) we're beginning to see what is possible when that infrastructure gap is addressed. Two recent examples illustrate the point.
Immunisation in Bay of Plenty
Bay of Plenty (BOP) has recorded some of the lowest immunisation rates in Aotearoa for years, making it a persistent focus for Health New Zealand's System Level Measures (SLM) programme. At the quarterly SLM review in February 2026, the data from Arataki's practices was striking.
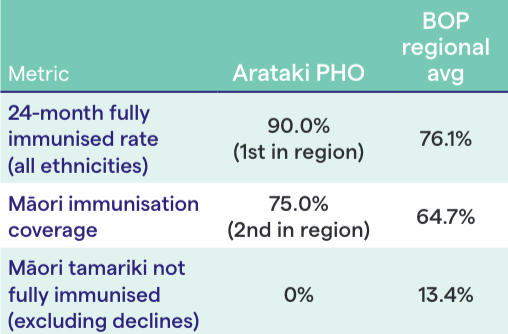
Our BOP practices achieved the highest 24-month fully immunised rate in the region across all ethnicities: 90% against a regional average of 76%. Māori immunisation coverages at at 75%, second in the region. And Arataki was the only PHO in Bay of Plenty with no Māori tamariki classified as not fully immunised (excluding firm declines).
These results didn't come from a single campaign. They reflect consistent, data-informed prioritised outreach: knowing which tamariki are due, which whānau need follow-up, and which communities face the greatest access barriers. That requires a data platform that surfaces answers in real time, not quarterly. The clinical teams did the work. The data infrastructure made sure they were reaching the right patients at the right time.
Measles response: directive to doorstep in 48 hours
That infrastructure was tested more acutely in October 2025 when measles re-emerged in Nelson with 11 confirmed cases, seven linked to a Bluebridge ferry crossing. Health New Zealand directed all PHOs to urgently boost vaccination rates.
Within 24 hours a multidisciplinary data and clinical team had built tools to identify unvaccinated patients stratified by risk: prioritising children under five, Māori and Pacific youth and people in high-deprivation areas. Within 48 hours, frontline nurses had prioritised lists in hand and were planning outreach. This wasn't a generic broadcast. It was targeted, evidence-led and fast.
The outreach was multi-channel: clinician-led video content in Te Reo Māori, English, and Mandarin; a patient messaging campaign achieving a 61% open rate; community partnerships; and walk-in immunisation clinics in high-needs areas including Eastgate Mall in Linwood, Christchurch.

The results above were measurable. Weekly MMR vaccinations rose from 32 per week to 189, a 5x increase. Conversions among previously vaccine-hesitant patients increased by 2.5x. And external vaccination records updated in practice management systems increased by 17x, reflecting a significant improvement in the data quality underpinning all future outreach.
"These results aren’t stories about one PHO performing well - they’re evidence of what becomes possible when primary care treats data as a crucial clinical tool, not just a reporting obligation. You can only close a gap when your systems are good enough to reveal it." - Josh Robb
The systemic gap this reveals
That last number matters more than it might appear. The measles response surfaced a significant challenge: adult vaccination records, particularly for overseas arrivals, are frequently incomplete or inaccessible. This isn't an Arataki problem - it's a sector-wide one. But you can only identify a data gap when your systems are good enough to reveal it.
This is the broader point. The sector's capacity challenges are real and well documented: workforce shortages, rising chronic disease burden, half a million New Zealanders not enrolled with a GP. Our ability to respond to these challenges depends fundamentally on data and digital infrastructure that most of the sector still lacks, particularly at the clinical frontline.
The investment required isn't glamorous. It's multidisciplinary teams with data engineering, system integration, analytics capability and the clinical knowledge and workflows that connect population-level insight to individual patient action. It's the kind of investment that health as historically undervalued compared to every other regulated industry I've worked in. But without it, we're making decisions within complete information, reacting to crises rather than anticipating them and measuring outcomes long after the opportunity to change them has passed.
Bay of Plenty's immunisation results and the measles response aren't stories about one PHO performing well. They're evidence of what becomes possible when primary care treats data as a crucial clinical tool rather than a reporting obligation.